One team. One plan. A new path.
NewPath is a not-for-profit run by nurses, a nurse practitioner, and people with lived experience of disability and mental health. Our model of care joins the medical model and the social model of disability into one plan and one team. A new path between the health system and everyday life, so nobody falls into the gap between them.
Why a model of care matters
In Australia, health care and disability support run as separate systems. When neither holds the whole picture, people with disability pay the price. In avoidable illness, avoidable hospital stays, and avoidable deaths.
38%
of deaths of people with intellectual disability are potentially avoidable. More than double the general population.1
3.5–4.5×
higher rates of preventable hospitalisation, for conditions good community care could have managed.2
72%
of hospitalised people with disability needing funded supports had their discharge delayed while systems argued over responsibility.3
These gaps aren't caused by bad people. They're caused by two half-pictures of the same person: a clinical lens that can miss the life, and a social lens that can miss the illness.
A change in behaviour gets blamed on "the disability" while an infection goes untreated. A discharge gets delayed for months while two systems decide whose job it is.
Each model is only half right
The classic example: a person who can't climb the stairs.
The medical model
"What's the condition? Let's treat it so they can climb the stairs."
It brings diagnosis, treatment, medication safety and clinical vigilance. It identifies illness, manages risk, and saves lives.
Alone, it falls short. A clinical lens can miss the life: the person's choices, goals, and the barriers around them.

The social model
"The stairs are the barrier. Build a ramp."
It brings rights, choice and control, inclusion and independence. This is the thinking behind the NDIS itself: disability is created by barriers, not by the person.
Alone, it falls short. A ramp doesn't manage epilepsy, pain, swallowing difficulty, dementia or depression. Real impairments still need skilled clinical care.
Build the ramp. And bring the nurse.
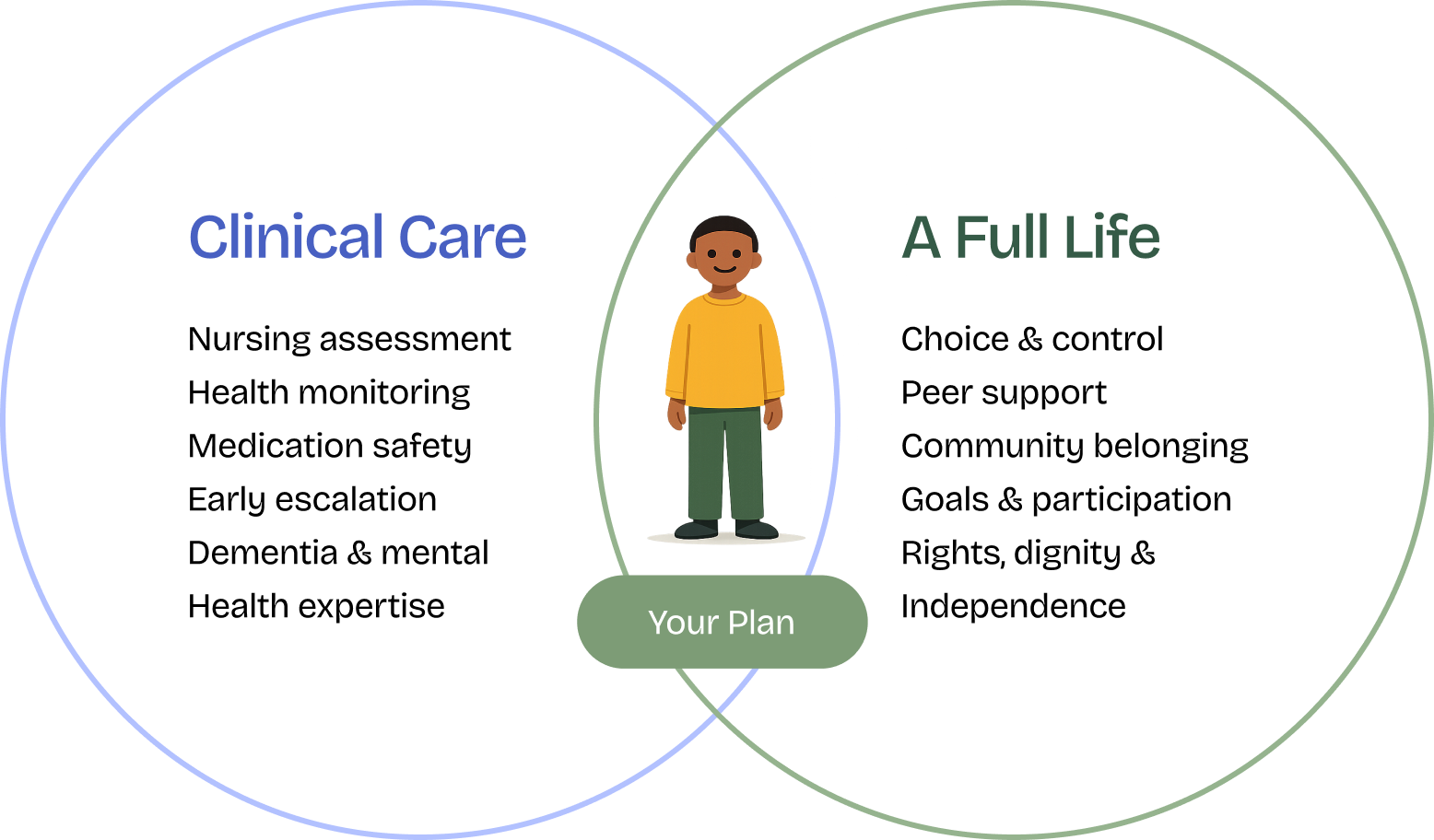
Our model follows the World Health Organization's ICF framework. It is the international standard that deliberately merges both models into one whole-of-person view: health, activity, participation and environment, all working together.7
Clinical care and a full life are not rivals. In our model, they meet in one plan: yours.
Five promises along the path
Nurse-led clinical governance
Registered Nurses and a Nurse Practitioner design and oversee every support plan. Health monitoring, medication awareness and early-deterioration alerts are built into everyday support, not bolted on after a crisis. Nurse-led care is linked to better self-management, satisfaction and fewer readmissions.8
Lived experience at every level
Peer support workers, staff with disability, and team members who have walked beside a family member through dementia or mental ill-health. Peer support is evidence-based, linked to hope, engagement and reduced hospitalisation.9 Here, lived experience shapes the whole organisation.
Recovery-oriented and person-led
We listen first and plan second. Your voice guides every decision. Our recovery coaching and support coordination practise hope and self-determination. Clinical knowledge serves your goals. It never overrides them.
One plan across systems
We speak both languages: clinical and NDIS. We work with hospitals on safe discharge, brief GPs properly, flag disability-related health supports, and end the "not our responsibility" hand-passing.3
Not-for-profit, by design
We're a registered charity. No shareholders and no profit margin steering decisions. Surpluses go back into training, smaller caseloads, and time with the people we support.
The people who walk alongside you
Support that feels human, not transactional. A team built so someone always holds the clinical picture, and someone has been where you are.
Registered Nurses
Clinical eyes on every plan.
Nurse Practitioner
Advanced clinical care.
Peer Support Workers
Lived experience of disability.
Family-carer team members
They've lived the journey too.
Your path with us, step by step
-
Connect
You, a family member, social worker, discharge planner or GP reaches out. We listen first.
-
See the whole you
One intake covering health, medications and risks. And goals, strengths, culture and barriers.
-
One plan
Clinical needs and life goals in a single plan, built with you and shared (with consent) across your GP and providers.
-
Support and watch closely
Workers who are clinically briefed and peer-informed, with nurse oversight to catch changes early.
-
Measure and adjust
We track what matters: goals, health stability, hospital avoidance, participation. And we adapt as life changes.
What this looks like when it counts
Real scenarios our referrers know well, and how an integrated, non-profit team responds differently.
Leaving hospital
The old way: the person waits weeks while health and NDIS argue over whose job the supports are.3
With NewPath: we engage before discharge, translate the clinical handover into the support plan, and have nurse-briefed workers ready on day one.
A change in behaviour or mood
The old way: it's blamed on "the disability", and a treatable infection, pain or depression is missed.1
With NewPath: support workers are trained to flag changes. A nurse reviews and escalates to the GP or Nurse Practitioner early.
Living with dementia
The old way: either over-medicalised, managed rather than living. Or under-supported, with no clinical monitoring as the condition progresses.
With NewPath: dignity-first daily support with structured clinical review as needs evolve. Home and connected, safely, for longer.
Psychosocial recovery
The old way: clinical services and NDIS supports run on parallel tracks, and the person retells their story endlessly.
With NewPath: a recovery coach fluent in both the mental health system and the NDIS holds one thread, with peer support alongside.
The outcomes we work toward
Built to deliver what the evidence says integrated, nurse-led, peer-informed care can achieve.8,9
- Fewer preventable hospitalisations, through early detection in everyday support
- Safer, faster hospital-to-home transitions, with supports ready on day one
- Stronger engagement and hope through peer support and recovery-oriented practice
- Real participation: goals achieved, community connection, independence on your terms
- Families genuinely informed, with one accountable point of contact
- Nothing about you, without you. Consent, choice and control at every step
Where to from here?
People with disability and families
You don't need all the answers. Just a starting point. We'll listen first, plan second, and walk beside you.
Medical practitioners
A clinically literate partner in the community: structured handover, health monitoring between appointments, and early escalation back to you. Referrals welcome from GPs, specialists and discharge planners.
Social workers and coordinators
We bridge the health and NDIS interface: discharge planning, disability-related health supports, and psychosocial recovery coaching. We hold the clinical picture and the person's goals together.
Sources and further reading
- Trollor J, Srasuebkul P, Xu H, Howlett S (2017), Cause of death and potentially avoidable deaths in Australian adults with intellectual disability using retrospective linked data, BMJ Open 7:e013489 (bmjopen.bmj.com); evidence to the Disability Royal Commission (2020).
- UNSW Sydney, Department of Developmental Disability Neuropsychiatry (2021), People with intellectual disability at "unacceptably high risk" of preventable hospitalisation (unsw.edu.au).
- Foster M et al. (2022), Planning with care complexity: factors related to discharge delays of hospitalised people with disability, Health & Social Care in the Community (pmc.ncbi.nlm.nih.gov); Summer Foundation, Hospital Discharge Position Statement (summerfoundation.org.au).
- Medical model of disability, overview and critiques: en.wikipedia.org/wiki/Medical_model_of_disability; Disability Nottinghamshire, Social Model vs Medical Model of Disability (disabilitynottinghamshire.org.uk).
- Social model of disability: en.wikipedia.org/wiki/Social_model_of_disability; National Disability Insurance Scheme Act 2013 (Cth) (legislation.gov.au).
- Reynolds JM (2017), Rethinking disability: the social model of disability and chronic disease (pmc.ncbi.nlm.nih.gov).
- World Health Organization (2001), International Classification of Functioning, Disability and Health (ICF) (who.int); WHO ICF overview (cdc.gov).
- Systematic reviews of nurse-led models of care in chronic and complex conditions (pmc.ncbi.nlm.nih.gov, 2025); Journal of Multidisciplinary Healthcare (2025).
- National Mental Health Commission, National Lived Experience (Peer) Workforce Development Guidelines (mentalhealthcommission.gov.au); umbrella review of peer-support effectiveness (pmc.ncbi.nlm.nih.gov, 2024).
Important information
General information only. The content on this page, including all statistics, illustrations, and descriptions of our model of care, is provided for general information purposes only. It does not constitute medical, clinical, legal, or financial advice, and it should not be relied upon as a substitute for advice from a qualified health professional who knows your circumstances. Always consult your GP or treating practitioner about your health, medications, or treatment. In an emergency, call Triple Zero (000). If you or someone you know needs crisis support, Lifeline is available 24/7 on 13 11 14.
About the research cited. Statistics on this page are drawn from the published, peer-reviewed research and government sources listed above. Each figure relates to the specific study population described in its source (for example, adults with intellectual disability, or hospitalised NDIS participants), and is presented to illustrate documented gaps between Australia's health and disability support systems. NewPath is not the author of this research, and the researchers and their institutions do not endorse NewPath.
About our services and outcomes. The outcomes described on this page are the goals our model of care works toward, informed by the evidence cited. They are not a guarantee of any particular result, and individual outcomes vary with each person's circumstances. Our services are subject to eligibility, funding arrangements, and availability, and are delivered in accordance with the NDIS Code of Conduct and applicable Australian law. NewPath is not a crisis or emergency service. Information about how we handle your personal information is in our Privacy Policy.
Copyright. © 2026 NEWPATH.ORG LTD (ABN 48 687 386 787), an Australian registered charity. All illustrations and text on this page are the property of NewPath and may not be reproduced without permission.
NewPath acknowledges the Traditional Owners of Country throughout Australia and recognises their continuing connection to land, waters and culture. We pay our respects to their Elders past, present and emerging.
Ready to walk a new path?
One team that holds the whole picture: your health, your goals, your life. Let's take the first step together.